Irritable Bowel Syndrome (IBS): Causes, Diagnosis, Treatment and How a Dietitian Can Help
- William Stivaletta

- Feb 19
- 4 min read

What Is Irritable Bowel Syndrome (IBS)?
Irritable Bowel Syndrome (IBS) is a functional gastrointestinal disorder, meaning that symptoms occur without visible structural damage to the digestive tract. IBS is commonly associated with:
Abdominal pain or discomfort
Bloating and excessive wind
Diarrhoea (IBS-D), constipation (IBS-C), or mixed bowel habits (IBS-M)
A sensation of incomplete bowel emptying
IBS is a long-term condition that can fluctuate over time and significantly affect quality of life, work performance, social activities, and mental wellbeing. It is estimated to affect between 5–20% of adults worldwide, making it one of the most common conditions seen in gastroenterology and dietetic practice .
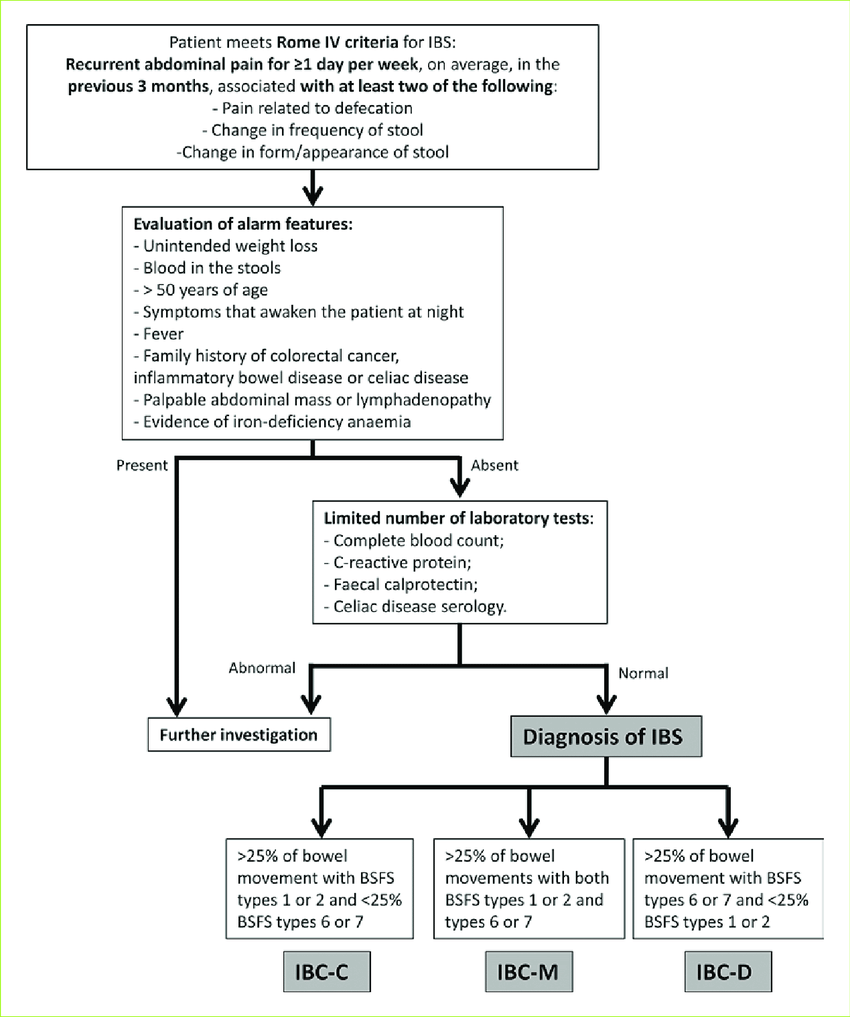
How Is IBS Diagnosed?

IBS is diagnosed based on symptom criteria (such as the Rome IV criteria) only after other conditions have been excluded. There is currently no single test that confirms IBS.
According to UK clinical guidance, individuals presenting with IBS-like symptoms should first be assessed to rule out:
Coeliac disease (via antibody blood tests)
Inflammatory bowel disease (IBD) using inflammatory markers and faecal calprotectin
Red-flag symptoms, including:
Unintentional weight loss
Anaemia
Rectal bleeding
Abdominal or rectal mass
Family history of bowel or ovarian cancer
Why IBS Is Often Overdiagnosed
In private and NHS settings alike, many people are diagnosed with IBS too quickly, without a comprehensive assessment. While IBS is common, similar symptoms can arise from multiple overlapping factors that may be missed if investigations stop too early.
These include:
Altered gut permeability
Chronic stress and nervous system dysregulation
Impaired digestion due to low stomach acid
Undiagnosed food intolerances
Gut microbiota imbalance (dysbiosis)
Being told “it’s just IBS” without exploring these contributors can leave patients feeling dismissed and unsupported.
IBS and the Gut–Brain Axis
The gut–brain axis describes the constant communication between the gastrointestinal tract and the central nervous system. Stress, anxiety, poor sleep, and prolonged psychological pressure can:

Increase gut sensitivity
Alter bowel motility (leading to diarrhoea or constipation)
Exacerbate bloating and abdominal pain
Influence gut bacteria composition
This explains why IBS symptoms often worsen during stressful life periods, even when diet remains unchanged. IBS is not psychological in origin, but stress can amplify gut symptoms through physiological pathways.
The Role of Digestion and Stomach Acid in IBS
Effective digestion begins in the stomach, where adequate stomach acid is essential for breaking down food and initiating the digestive process. When stomach acid production is reduced, digestion becomes less efficient, particularly for protein-rich foods. This can result in incomplete digestion, allowing partially broken-down food to pass into the intestines, where it is more likely to ferment.
Poor digestion increases the amount of undigested material reaching the large intestine. Here, gut bacteria ferment these substances, producing gas and other by-products that can contribute to bloating, abdominal discomfort, reflux-like symptoms, and changes in bowel habit. Factors such as meal timing, portion size, eating speed, and overall food composition all play a role in how effectively food is digested. Large meals, irregular eating patterns, or eating quickly under stress can place additional strain on the digestive system and exacerbate IBS symptoms.
Gut Dysbiosis and IBS Symptoms
Many people with IBS experience gut dysbiosis, an imbalance between beneficial and gas-producing bacteria. This can increase:
Gas production
Bloating and abdominal pressure
Sensitivity of the gut wall
Certain carbohydrates known as FODMAPs (Fermentable Oligo-, Di-, Mono-saccharides And Polyols) are poorly absorbed and rapidly fermented, which can worsen symptoms in susceptible individuals .
IBS Treatment: What Actually Helps?
IBS has no single cure, but symptoms can be effectively managed with a structured, evidence-based approach.
First-line management includes:
Regular meals
Adequate hydration
Reducing caffeine and alcohol
Adjusting fibre intake
Increasing physical activity
If symptoms persist, second-line dietary strategies, such as the low FODMAP diet, may be introduced under dietetic supervision. This approach involves structured restriction, reintroduction, and long-term personalisation to avoid unnecessary food avoidance .
How a Dietitian Can Help with IBS
A registered dietitian plays a central role in IBS management by:
Ensuring IBS is an appropriate diagnosis
Identifying dietary triggers safely and systematically
Supporting evidence-based approaches such as the low FODMAP diet
Preventing nutritional deficiencies
Addressing lifestyle factors, stress, and eating behaviours
In private practice, dietetic support focuses on individualised care, realistic goal-setting, and sustainable symptom improvement not overly restrictive diets or quick fixes.
Key Takeaway
IBS is a real, complex, and multifactorial condition. Effective management requires more than removing foods—it requires understanding the interaction between diet, digestion, gut bacteria, stress, and lifestyle.
A personalised dietetic approach can significantly improve symptoms and quality of life, even when IBS has been present for years.
References
NICE. Irritable bowel syndrome in adults: diagnosis and management (CG61). Updated 2017.
British Society of Gastroenterology. Guidelines on the management of irritable bowel syndrome. Gut, 2021.
McKenzie YA et al. British Dietetic Association evidence-based guidelines for the dietary management of IBS. J Hum Nutr Diet, 2016.
Whelan K. The role of FODMAPs in IBS. J Hum Nutr Diet, 2017.
Schumann D et al. Yoga vs low FODMAP diet in IBS: a randomised clinical trial. Aliment Pharmacol Ther, 2018.
Staudacher HM et al. Mechanisms of action of FODMAPs in IBS. Gut, 2017.



Comments